
Disease Information
What is MOGAD?
Myelin oligodendrocyte glycoprotein antibody-associated diseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease (MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease ) is a rare inflammatory disease of the central nervous systemNerve tissue that resides in and composes the brain, spinal cord, and optic nerve (CNSNerve tissue that resides in and composes the brain, spinal cord, and optic nerve). In MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , the immune system attacks the protective coating around nerve fibers, called myelinAn insulating layer, or sheath that forms around nerves, including those in the brain and spinal cord. It is made up of protein and fatty substances. This myelin sheath allows electrical impulses to transmit quickly and efficiently along the nerve cells. If myelin is damaged, these impulses slow down., leading to damage in areas like the optic nervesThe cranial nerves that relay messages from your eyes to your brain to create visual images. These nerves extend from the retina in the back of the eyes to the part of the brain that processes what we see. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), they may be the target of inflammation or lesions, sometimes causing visual disruption or blindness., brain, and/or spinal cord1.
How does MOGAD Develop?
While the exact cause of MOGAD is unknown, it is thought to be caused by autoantibodies known as myelin oligodendrocyte glycoprotein immunoglobulin G (MOG-IgG)Refers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system, which are antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. in the immune system that mistakenly target healthy proteins in the body2. In MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , these autoantibodies cause damage to healthy MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. proteins onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. the outer protective surface of nerve cells, leading to demyelinationThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems.1,3. DemyelinationThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. can be compared to a power cord onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. a lamp short-circuiting when its protective plastic coating is stripped away. Without this insulation, the flow of electricity is disrupted, causing the lamp to flicker or fail to work. Similarly, in MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , the loss of myelinAn insulating layer, or sheath that forms around nerves, including those in the brain and spinal cord. It is made up of protein and fatty substances. This myelin sheath allows electrical impulses to transmit quickly and efficiently along the nerve cells. If myelin is damaged, these impulses slow down. impairs nerve signal transmission, leading to disruptions in nerve function4.
Recently, doctors have recognized that MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease is a distinct disease, separate from other neurological conditions like Neuromyelitis Optica Spectrum DisorderA disorder of the central nervous system that primarily affects the nerves of the eye and the spinal cord. Also known as Neuromyelitis Optica (NMO) or Devic’s Disease (NMOSDA disorder of the central nervous system that primarily affects the nerves of the eye and the spinal cord. Also known as Neuromyelitis Optica (NMO) or Devic’s Disease), Chronic Relapsing Inflammatory Optic Neuropathy (CRION)A disease where the optic nerve is the target of two or more demyelinating attacks separated by at least 30 days, resulting in visual deficits and may or may not be accompanied by pain on eye movement. CRION patients may or may not be MOG antibody positive. and Multiple SclerosisAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve. (MSAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve.). Although these conditions can have similar symptoms, improved testing for MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. has made it easier to accurately diagnose MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease and tell it apart from other demyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. diseases of the CNSNerve tissue that resides in and composes the brain, spinal cord, and optic nerve5-6.
Who is affected by MOGAD?
Prevalence and incidence of MOGAD is still being studied, and the exact numbers can vary by region. However, research from different parts of the world shows that MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease is relatively rare. Estimates suggest that about 1.3 to 2.5 people per 100,000 have MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , and each year, there are around 3.4-4.8 new cases per million people7.
Although MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease affects both men and women, and can happen at any age, it most commonly presents in those 28-30 years of age7. Around 30% of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease cases occur in children, making it one of the more common causes of acquired central nervous systemNerve tissue that resides in and composes the brain, spinal cord, and optic nerve (CNSNerve tissue that resides in and composes the brain, spinal cord, and optic nerve) demyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. syndromes in young people8. Currently, unlike MSAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve. and NMOSDA disorder of the central nervous system that primarily affects the nerves of the eye and the spinal cord. Also known as Neuromyelitis Optica (NMO) or Devic’s Disease, MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease shows no clear racial preponderance or strong human leucocyte antigen associations, though further research is needed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. how ethnicity may influence MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease expression8,9. As doctors become more familiar with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease and testing becomes more widely available, it’s likely that more cases will be diagnosed in the future7.
Signs & Symptoms
MOGAD typically presents as a sudden onset of symptoms, referred to as an acuteThe severe and sudden onset of a disease process. attack, which can vary in type and severity. It can also vary in how it presents over one’s lifetime, where it can be multiphasicA disease characterized by two or more phases or attacks. (relapsing) or monophasicA disease characterized by only one phase or attack.10,11,12.
- MultiphasicA disease characterized by two or more phases or attacks.: characterized by recurrent attacks following the initial episode
- MonophasicA disease characterized by only one phase or attack.: an individual experiences only a single attack throughout their lifetime13.
MonophasicA disease characterized by only one phase or attack. classification represents approximately 50% of MOGAD cases. Emerging research suggests that young adults (below the age of 40) have a higher risk of relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). compared to those above the age of 408,14. However, the classification of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease as monophasicA disease characterized by only one phase or attack. has recently been challenged, and further research is needed. It is suggested that MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease may predominantly be a relapsing disease when observed over a longer follow-up period, with the monophasic nature of some individuals possibly being an artifact of insufficient observation time8.
Individuals with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease may have varying levels of MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system over time, and higher titers are associated with a higher likelihood of an accurate diagnosis, as these elevated levels are more detectable in tests15,16. Increased MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system titers enhance diagnostic sensitivity, helping differentiate MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease from other demyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. conditions15,16. Additionally, fluctuations in MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system levels can reflect disease progression and treatment response, providing valuable insights into disease activity and guiding therapeutic decisions15,16,17.

Optic Neuritis (ON)
ON is the most common symptom of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease in adults and is characterized by inflammation of the optic nerve, often presenting as severe
headaches or orbital pain. Additional symptoms associated with ON may include:
- Blurry vision
- Vision loss
- Double vision
- Peripheral vision loss
- Color vision loss
- Optical disc edema
ONInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. can occur unilaterally, affecting one eye, or more commonly, bilaterally, affecting both eyes (Li et al., 2022; Rempe et al., 2021).
Transverse Myelitis (TM)
TM, another common manifestation of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , may occur alone or in conjunction with ON, and is characterized by inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. of the spinal
cord which may cause:
- Abnormal sensations such as numbness, tingling, burning, coldness, squeezing, electric shock, shooting pain, or itching
- Muscle weakness
- Loss of motor control
- Bladder and bowel control issues
- Stiff or weak muscles
- Muscle spasms
- Sexual dysfunction (Li et al., 2022)
Acute Disseminated Encephalomyelitis (ADEM)
ADEMAn initial and brief autoimmune attack that causes widespread inflammation and damage to the brain, spinal cord, and optic nerve, typically in children. This initial attack establishes the basis for diagnosis. The MOG antibody is detectable in a percentage of Acute Disseminated Encephalomyelitis (ADEM) patients. involves a brief but widespread attack of inflammation in the brain and spinal cord, which can lead to the rapid onset of symptoms such as:
- Confusion
- Difficulty swallowing
- Loss of coordination
- Loss of balance
- Headaches
- Behavioral changes
- Loss of consciousness
- SeizuresA sudden, temporary disturbance in brain activity that causes changes in behavior, movement, sensation, or consciousness (Li et al., 2022)
Autoimmune Encephalitis (AE)
Autoimmune encephalitis (AE)Encephalitis caused by an immune attack on the brain (as opposed to viral encephalitis). Refer to encephalitis., or inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. of the brain, is another manifestation of MOGAD. It can lead to symptoms such as:
- Fever
- Impairment or loss of consciousness
- Seizures
- Loss of coordination
- Behavioral changes (Hegen et al., 2020)
Cerebral Cortical Encephalitis (CCE)
Until recently, encephalitisA disease in which inflammation of brain tissue caused by an infection or an autoimmune response results in swelling and damage. When caused by an autoimmune disease, sometimes called Autoimmune Encephalitis. in MOGAD was believed to affect subcortical structures, similar to ADEM. However, a rare and distinct form of MOGAD-related encephalitisA disease in which inflammation of brain tissue caused by an infection or an autoimmune response results in swelling and damage. When caused by an autoimmune disease, sometimes called Autoimmune Encephalitis. has recently been identified, known as cerebral cortical encephalitisA disease in which inflammation of brain tissue caused by an infection or an autoimmune response results in swelling and damage. When caused by an autoimmune disease, sometimes called Autoimmune Encephalitis. (CCEA rare clinical phenotype of MOGAD, which usually begins with seizures, headaches, and fever. Sometimes there is only one-sided cerebral cortical inflammation without any white matter inflammation. MOGAD patients who experience this phenotype are often misdiagnosed with viral encephalitis, stroke or infection.), which is characterized by FLAIR (Fluid attenuate inversion recovery)-hyperintense Lesions in Anti-MOG-associated EncephalitisA disease in which inflammation of brain tissue caused by an infection or an autoimmune response results in swelling and damage. When caused by an autoimmune disease, sometimes called Autoimmune Encephalitis. with SeizuresA sudden, temporary disturbance in brain activity that causes changes in behavior, movement, sensation, or consciousness (FLAMES). The most common clinical symptoms of FLAMES include:
- SeizuresA sudden, temporary disturbance in brain activity that causes changes in behavior, movement, sensation, or consciousness
- Headaches
- Fevers
- Cortical symptoms related to the affected brain area (Ogawa et al., 2017; Valencia-Sanchez et al., 2022; Maturu et al., 2023)
Diagnosis
Diagnosing MOGAD based on symptoms alone can be challenging due to the similarities with NMOSD, CRIONA disease where the optic nerve is the target of two or more demyelinating attacks separated by at least 30 days, resulting in visual deficits and may or may not be accompanied by pain on eye movement. CRION patients may or may not be MOG antibody positive. and MS10. To establish a diagnosis, these other conditions must be excluded. Many individuals living with MOGAD may have previously been misdiagnosed with atypical MS or seronegative NMOSDA disorder of the central nervous system that primarily affects the nerves of the eye and the spinal cord. Also known as Neuromyelitis Optica (NMO) or Devic’s Disease or CRION, however are now considered to have MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease with a distinct clinical presentation8. This requires a careful differential diagnosis using clinical symptoms, laboratory results, and imaging findings. Prompt testing, especially in the acuteThe severe and sudden onset of a disease process. phase of the disease, is critical for an accurate diagnosis and timely treatment, which can help improve outcomes for individuals living with MOGAD34.
For more information onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. the diagnostic criteria please visit the following page: https://mogproject.org/demystifying-the-diagnosis-of-mogad-take-home-points-for-patients-from-the-2023-international-mogad-panel-proposed-diagnostic-criteria/
MOG-IgG Testing
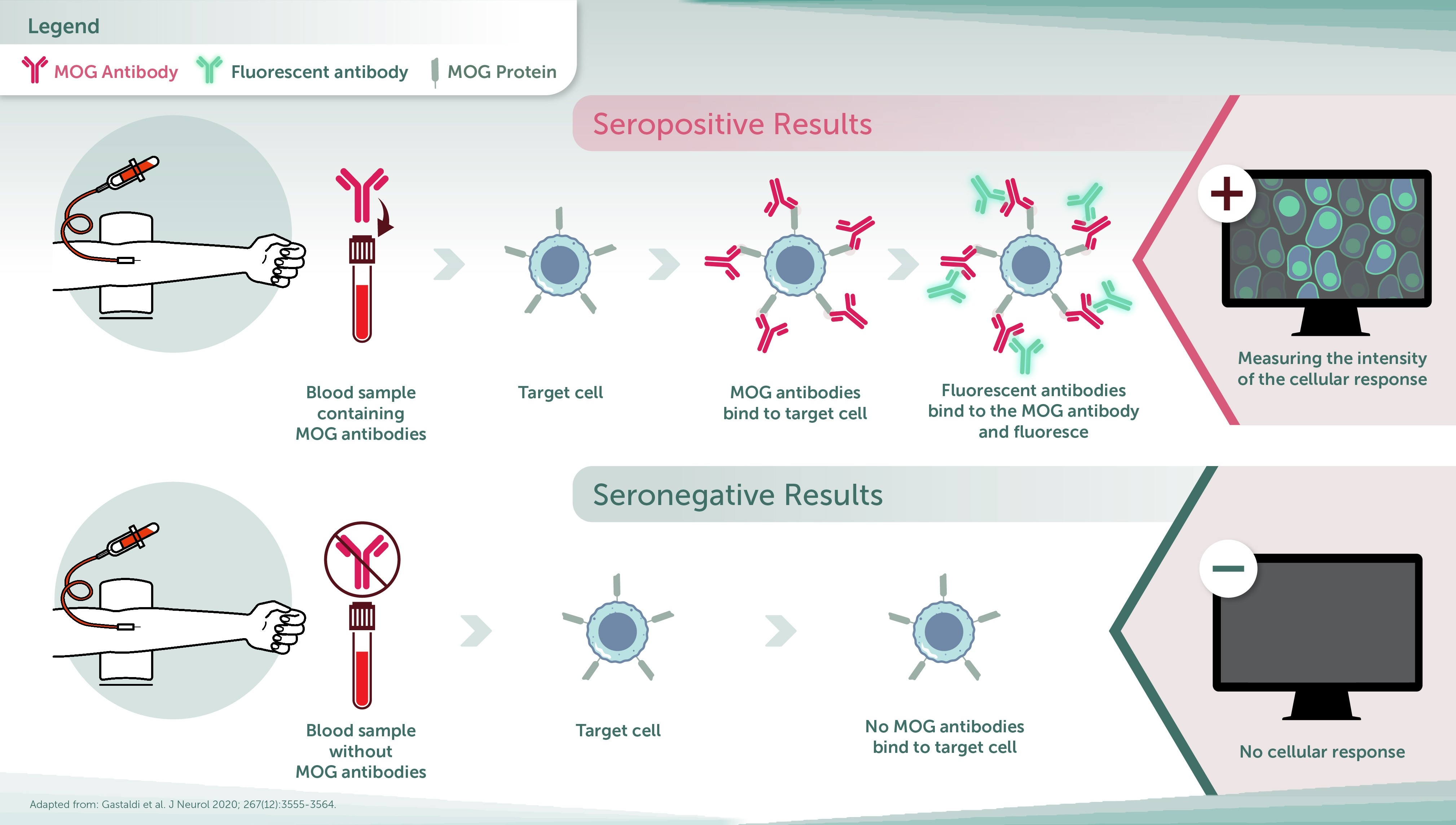
The most important criterion for MOGAD diagnosis is the presence of MOG-IgG antibodies. These antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. can be detected in blood or cerebrospinal fluid (CSF), and their presence is a key marker for MOGAD. Below are key points related to the testing process for these antibodies:
- Serum testing is the most common method
- The live cell-based assayA laboratory test used to: • Measure the presence or amount of a specific substance: in a sample, such as blood, urine, or tissue.
• Determine the potency or activity: of a drug or other substance.
• Analyze the purity: of a chemical compound.
• Identify and quantify: biomarkers related to a disease or condition.
is the gold standard for testing MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system levels yet must be done prior to any treatment5. - MOG-IgG levels may decrease over time following an acuteThe severe and sudden onset of a disease process. attack, which can result in false negative results.
- For this reason, testing should be performed promptly after the onset of symptoms and repeated if necessary35.
- CSF analysis may be useful when blood tests yield inconclusive results
- MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system has been found in CSFA clear, colorless liquid found throughout the cavities of the central nervous system that helps protect the brain and spinal cord by acting like a cushion against sudden impact or injury, and provides a medium for the transport of nutrients and the removal of waste products for proper functioning. of 12% of individuals who are seronegative yet present with symptoms of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , however this presence may be indicative of a more severe clinical presentation36,37,38.
However, the presence of MOG-IgG antibodiesRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system alone is not sufficient for a diagnosis, as antibodyA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. levels can fluctuate over time, and low levels may result in false-positives or negatives15.
Imaging
- Magnetic Resonance Imaging (MRI) is crucial in assessing inflammation and/or lesions in the optic nerves, spinal cord, and brain, which are commonly seen in MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease 5.
- However, in about 10% of cases, MRIA noninvasive imaging technique that uses strong magnetic fields to produce images of nearly any structure of the body. For MOGAD, it is typically used with and without contrast to identify disease activity in the central nervous system. findings may initially appear normal at the onset of symptoms, even when individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease experience significant clinical disability and repeat MRIA noninvasive imaging technique that uses strong magnetic fields to produce images of nearly any structure of the body. For MOGAD, it is typically used with and without contrast to identify disease activity in the central nervous system. after days/weeks may be necessary39.
- Optical coherence tomography (OCT) is often performed for evaluating optic nerveThe cranial nerves that relay messages from your eyes to your brain to create visual images. These nerves extend from the retina in the back of the eyes to the part of the brain that processes what we see. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), they may be the target of inflammation or lesions, sometimes causing visual disruption or blindness. damage, which allows for direct visualization of the nerve’s condition.
- Visual field testing can also be used to detect blind spots or other visual impairments caused by optic neuritisInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement.5,40.
Treatments: Acute and Preventative Care
Although there are currently no FDA-approved treatments specifically for MOGAD, various therapies can help manage symptoms, reduce relapses and control inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths.5. Treatment strategies vary depending on whether the individual is in the acuteThe severe and sudden onset of a disease process. phase or needs long-term preventiveRefers to a medication or treatment that is administered to prevent future relapses (Also referred to as Preventative or Preventive Treatment). care.
Acute Treatment
During the acute phase, the primary goal is to reduce inflammation and prevent further damage by targeting and lowering the levels of MOG-IgG antibodies. High-dose corticosteroids are typically the first-line treatment, administered either orally or intravenouslyA way of giving a drug or other substance through a needle or tube inserted into a vein.. These steroidsA type of medication typically given intraveneously or orally. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD) it is used as an immunosuppressant and anti-inflammatory to reduce disease activity and inflammation. In adults, it is sometimes used in high doses for acute attacks. In some adult patients, it may be used for 1-2 months after an acute attack to avoid a rapid onset of relapse. Higher doses (>10mg/day) are not recommended for an extended period of time but lower doses (<=10mg/day) may be used in some patients longer term. In children, it may be used after treatment of an acute attack, but it is not recommended long-term due to the profound effects of chronic steroids on a child’s health. Use of oral prednisone as a maintenance therapy in relapsing pediatric MOGAD patients is discouraged due to side effects in developing children, and other therapies such as monthly immune globulin are suggested. (To understand relapsing during steroid tapering, see Steroid Dependency) work by suppressing the immune system and reducing inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths.. However, prolonged use of corticosteroids can lead to steroid dependency and other side effects such as weight gain, elevated blood pressure, elevated blood sugar, cataracts, insomnia, osteoporosis, edema, heart rhythm abnormalities, muscle atrophy and more5,40. As such, after the initial acute attack, steroid tapering may be performed to gradually reduce the dosage of corticosteroids to minimize side effects while continuing to suppress inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths.. Steroid tapering must be done carefully to avoid a rebound increase in inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths..
In some cases, additional treatments may be used in combination with or in place of steroids. This may include:
- Plasma exchangeA procedure in which a machine is used to separate the patient’s plasma from the blood cells. The plasma is separated from the blood cells, the blood cells are mixed with a liquid to replace the plasma, then it is returned to the patient’s body. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this treatment is sometimes given to remove antibodies from the blood stream to reduce disease activity during an active attack. May be used as a preventative treatment when other treatment options fail. (PLEXA procedure in which a machine is used to separate the patient’s plasma from the blood cells. The plasma is separated from the blood cells, the blood cells are mixed with a liquid to replace the plasma, then it is returned to the patient’s body. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this treatment is sometimes given to remove antibodies from the blood stream to reduce disease activity during an active attack. May be used as a preventative treatment when other treatment options fail./ plasmapheresisA procedure in which a machine is used to separate the patient’s plasma from the blood cells. The plasma is separated from the blood cells, the blood cells are mixed with a liquid to replace the plasma, then it is returned to the patient’s body. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this treatment is sometimes given to remove antibodies from the blood stream to reduce disease activity during an active attack. May be used as a preventative treatment when other treatment options fail.) can be performed to remove harmful MOG-IgG antibodiesRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system from the blood, offering additional immune modulation5,41. For risks/ side effects of PLEXA procedure in which a machine is used to separate the patient’s plasma from the blood cells. The plasma is separated from the blood cells, the blood cells are mixed with a liquid to replace the plasma, then it is returned to the patient’s body. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this treatment is sometimes given to remove antibodies from the blood stream to reduce disease activity during an active attack. May be used as a preventative treatment when other treatment options fail., please see the following resources:
- Corticosteroids help reduce inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. and supress the immune response from the acuteThe severe and sudden onset of a disease process. attack5,40. For the risks/ side effects of corticosteroids, please see the following resources:
- IntravenousA way of giving a drug or other substance through a needle or tube inserted into a vein. immunoglobulinA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment. (IVIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment.) involves infusing antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. from healthy donors. The mechanism of action of IVIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment. is not fully understood but is thought to involve enhanced clearance and interference with MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system., as well as modulation of the immune response5,42. For the risks/ side effects of IVIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment., please see the following resource:
Preventative Treatment
For individuals living with MOGAD who have a history of relapse, preventiveRefers to a medication or treatment that is administered to prevent future relapses (Also referred to as Preventative or Preventive Treatment). treatments are typically recommended to avoid further relapses and minimize the risk of long-term disability.
After a first MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease attack, the decision to initiate long-term, preventiveRefers to a medication or treatment that is administered to prevent future relapses (Also referred to as Preventative or Preventive Treatment). therapy depends on how the individual responds to acute treatmentA type of treatment that is intended to stop an ongoing attack., the level of damage from the initial attack, and the risk for further relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community).. In about 33% of individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , it is a one-time occurrence, with only one attack in their lifetime5,8,15. If the response to acute treatmentA type of treatment that is intended to stop an ongoing attack. after an initial attack is complete and MOG-IgG levels are undetectable, doctors may opt to delay long-term treatment until a second attack occurs. However, if the response to treatment is incomplete, and MOG-IgG levels remain elevated, immunomodulatorsA substance that affects the function of the immune system, either stimulating or suppressing its activity may be recommended to prevent further relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). and minimize the risk of long-term disability. While there is no defined biomarker indicative of relapse in MOGAD, some physicians may recommend not to risk a second attack and initiate preventativeRefers to a medication or treatment that is administered to prevent future relapses (Also referred to as Preventative or Preventive Treatment). treatment to avoid further damage. Risks of adverse effects from immunosuppressive therapies also need to be taken into consideration. These discussions should be individualized, and shared decision making between the physician and the patient is essential. Treatments to prevent MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). may include:
- ImmunomodulatorsA substance that affects the function of the immune system, either stimulating or suppressing its activity such as mycophenolate mofetilCellCept is the brand name for Mycophenolate Mofetil (also sometimes referred to as MMF). It is an immunosuppressant medication often prescribed for some autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity., rituximabThe common brand for this drug is Rituxan. A therapeutic drug that suppresses the immune system often prescribed in certain autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity.43, tocilizumabAn immunosuppressive drug that blocks the inflammatory protein IL-6. This may improve symptoms caused by inflammation. The common brand for this drug is Actemra. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity. May be given intraveneously or by subcutaneous injection. and azathioprineBrand names include Imuran and AZT. A therapeutic drug that suppresses the immune system often prescribed in certain autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity.40,44. These are used to reduce inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. and prevent future attacks. For more information regarding the efficacy and side effects of immunomodulatorsA substance that affects the function of the immune system, either stimulating or suppressing its activity, please see the following resources:
- Mycophenolate mofetilCellCept is the brand name for Mycophenolate Mofetil (also sometimes referred to as MMF). It is an immunosuppressant medication often prescribed for some autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity.:
- RituximabThe common brand for this drug is Rituxan. A therapeutic drug that suppresses the immune system often prescribed in certain autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity.:
- Efficacy: https://pmc.ncbi.nlm.nih.gov/articles/PMC9728038/#abstract1
- Risks/ side effects: https://www.drugs.com/rituximab.html#side-effects
- TocilizumabAn immunosuppressive drug that blocks the inflammatory protein IL-6. This may improve symptoms caused by inflammation. The common brand for this drug is Actemra. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity. May be given intraveneously or by subcutaneous injection.:
- AzathioprineBrand names include Imuran and AZT. A therapeutic drug that suppresses the immune system often prescribed in certain autoimmune conditions. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity.:
- IntravenousA way of giving a drug or other substance through a needle or tube inserted into a vein. immunoglobulinA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment. (IVIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment.) or subcutaneousA method of administering medication by injection under the skin. immunoglobulinA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment. (SCIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment.), which involves regular infusions of antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. from healthy donors45. These treatments help neutralize MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. and decrease the immune response that triggers relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community)., proving highly effective when administered at the correct dosage and interval5,46,47.
- Low-dose oral corticosteroids may be used for short periods following an attack and are sometimes taken in low doses long-term to prevent relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in adults, though this treatment is not typically prescribed for children given the risks for adverse effects5,46.
Long-term management of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease often involves a combination of these therapies to balance controlling inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. and minimizing the side effects of chronic treatment5. Individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease are unresponsive to conventional MSAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve. therapies like interferon beta and glatiramer, making accurate MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease diagnosis crucial for effective treatment44.
Ongoing Clinical Trials
Several promising treatments are currently being investigated in clinical trials. These treatments include:
- Neonatal Fc receptor inhibitor (FcRn), rozanolixizumab. By blocking FcRn, which normally helps preserve MOG-IgG antibodiesRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system in the body, rozanolixizumab accelerates the degradation of MOG-IgG antibodiesRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system, thereby reducing the immune response48,49. Rozanolixizumab is currently in Phase 3 of clinical trials1.
- Rozanolixizumab (cosMOG): This randomized, double-blind, placebo-controlled, multicenter study is designed to assess the efficacy and safety of rozanolixizumab in adult patients aged 18 to 89 with at least one relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in the past 12 months. The study will include 104 participants worldwide and began onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. February 2, 2022, with an expected completion date of July 1, 2027.
For more details: https://mogproject.org/clinical-trials/#cosmog
- IL-6 receptor targeted drugs, satralizumab and tocilizumabAn immunosuppressive drug that blocks the inflammatory protein IL-6. This may improve symptoms caused by inflammation. The common brand for this drug is Actemra. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity. May be given intraveneously or by subcutaneous injection., which work to suppress the immune response involved in MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease attacks. These are in Phase 3 and Phase 2/3 of clinical trials, respectively50,51,52,53.
- Satralizumab (METEOROID): This randomized, double-blind, placebo-controlled, multicenter study aims to evaluate the efficacy, safety, pharmacokineticsThe branch of pharmacology concerned with the movement of drugs within the body., and pharmacodynamicsThe study of what a drug does to the body, essentially examining the effects of drugs on living systems. of satralizumab in patients aged 12 years or older with a confirmed diagnosis of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease . Eligible participants must have experienced at least one relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in the past 12 months or at least 2 attacks in the past 24 months. The trial, involving 152 participants worldwide, began onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. August 30, 2022, and is set to conclude onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. December 31, 2028.
For more details: https://mogproject.org/clinical-trials/#meteoroid
- TocilizumabAn immunosuppressive drug that blocks the inflammatory protein IL-6. This may improve symptoms caused by inflammation. The common brand for this drug is Actemra. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity. May be given intraveneously or by subcutaneous injection. (TOMATO): This randomized, controlled multicenter study aims to evaluate the safety and efficacy of tocilizumabAn immunosuppressive drug that blocks the inflammatory protein IL-6. This may improve symptoms caused by inflammation. The common brand for this drug is Actemra. For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), this medication is used to suppress the immune system to reduce disease activity. May be given intraveneously or by subcutaneous injection. in patients aged 12 years or older with a confirmed diagnosis of MOGAD. Eligible participants must have experienced at least one relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in the past 12 months or at least 2 attacks in the past 24 months. The trial, involving 102 participants in China, began on July 9, 2024, and is set to conclude onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. July 1, 2026.
For more details: https://clinicaltrials.gov/study/NCT06452537?intr=tocilizumab&cond=MOGAD&rank=1
Prognosis and Understanding Relapsing Disease
The prognosis for individuals with MOGAD can vary significantly, making it difficult to predict the likelihood of relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community)., their severity, and the extent of recovery following subsequent attacks11. While it’s suggested that approximately 67% of individuals experience relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community)., it is uncertain who will relapse or when these relapses might happen8. Understanding relapse patterns is crucial for managing the long-term course of the disease and improving patient outcomes.
Risk Factors for RelapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community).
Tracking relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). patterns over time is crucial for assessing the progression of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease , as accumulated disability is believed to result from relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). rather than continuous progression8. Certain factors have been associated with an increased risk of relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease :
- Age: Older children17.
- Gender: Female54.
- Ethnicity: Hispanic/Latino54.
- Initial symptoms: Individuals presenting with ON as an initial symptom17.
- Presence of the non-p42 epitope in patients particularly with an ONInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. phenotypeWhen used in reference to myelin oligodendrocyte glycoproten antibody disease (MOGAD), indicates the particular presentation or combination of symptoms an individual experiences based on the part of the central nervous system affected by MOGAD. is the first serological marker that may be indicative of relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community).55.
- Seropositivity: Persistent seropositivity (the presence of MOG-IgG antibodiesRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system) in blood tests after an acuteThe severe and sudden onset of a disease process. attack may indicate a higher risk of relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). in some individuals15,17. However, patients who become seronegative can return to seropositiveA laboratory test result that shows the presence of a specific marker, usually an antibody, in the blood. For MOGAD, seropositive means that you have tested positive for the MOG antibody. and experience an attack, and some patients who remain seropositiveA laboratory test result that shows the presence of a specific marker, usually an antibody, in the blood. For MOGAD, seropositive means that you have tested positive for the MOG antibody. do not have relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community).56.
Importance of Early Diagnosis and Relapse Management
Getting an early diagnosis of MOGAD and prompt treatment following the first attack is crucial for preparing individuals living with MOGAD for the possibility of future relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community).57,58. MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease attacks, especially those involving the spinal cord (myelitis and ADEM), can cause significant neurological damage that may be permanent, leading to long-term disability12. Individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease who experience myelitis during their initial attack are at higher risk of enduring long-term functional impairments12.
For individuals at high risk of relapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community)., ongoing preventiveRefers to a medication or treatment that is administered to prevent future relapses (Also referred to as Preventative or Preventive Treatment). treatment, such as those described above, have been shown to reduce the likelihood of future relapses54. Interestingly, ONInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. is the most common symptom observed during relapse, regardless of the symptoms during the initial attack40.
Early intervention and prompt treatment during relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). can help prevent new and permanent damage to the nervous system, which in turn may minimize long-term disability and improve the overall prognosis for individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease . In some instances, this swift treatment allows patients to recover partially or entirely back to their pre-attack baseline57.
A pseudo-relapseThe recurrence of neurologic symptoms often due to an exacerbating factor or trigger such as heat or sickness. Pseudo-relapses can often be distinguished clinically from relapses by their fluctuance in severity and improvement over 24-48 hours. Pseudo-relapses will never show any new or worsening lesions on MRI. in MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease refers to the temporary recurrence or worsening of neurological symptoms, often triggered by external factors such as heat, stress, infections, or other physical or emotional stressors. Unlike true relapses, pseudo-relapses are characterized by their transient nature, with symptoms fluctuating in severity and typically improving within 24-48 hours. Clinically, pseudo-relapses can be distinguished from genuine relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). by the absence of new or worsening lesions onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. MRIA noninvasive imaging technique that uses strong magnetic fields to produce images of nearly any structure of the body. For MOGAD, it is typically used with and without contrast to identify disease activity in the central nervous system., indicating that they do not reflect disease progression. However, physicians must exercise caution in making this distinction if there is an exam change, as relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). can occasionally occur despite negative MRIA noninvasive imaging technique that uses strong magnetic fields to produce images of nearly any structure of the body. For MOGAD, it is typically used with and without contrast to identify disease activity in the central nervous system. findings59. Pseudo-relapses are thought to result from factors that exacerbate existing symptoms without triggering active inflammationA process of the immune system that involves chemicals released by immune cells (i.e. white blood cells) inducing localized heat, swelling, redness, and pain to an area that occurs when tissue becomes damaged or infected from a pathogen, and usually results in the desctruction and removal of the pathogen and/or healing to the tissue. In the case of myelin oligodendrocyte glycoprotein antibody disease (MOGAD), inflammation is the result of the incorrect targeting of the myelin oligodendrocyte glycoprotein (MOG) by the immune system, resulting in damage to myelin sheaths. or demyelinationThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. in the central nervous system (CNS)Nerve tissue that resides in and composes the brain, spinal cord, and optic nerve.
Impact on Quality of Life
Being diagnosed with MOGAD can affect an individual’s quality of life (QoL). The physical symptoms of an attack, such as vision impairment, mobility issues and weakness can interfere with daily activities and limit a person’s independence. These limitations may affect an individual living with MOGAD’s ability to:
- Maintain employment
- Manage personal care
- Engage in social or recreational activities
In addition to the physical impact, mental health challenges are common among individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease . Studies have found that these individuals may experience heightened:
- Anxiety60
- Depression60
- Fatigue31
- Cognitive difficulties60
- Social isolation60
These psychological and emotional burdens often compound the physical challenges of the disease, making effective management of MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease essential not just for preventing relapsesWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community)., but also for improving overall well-being.
Please see these helpful resources to support living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease :
- Education:
- Disease Information: https://mogproject.org/resources/
- Facts Sheets, Patient Brochure, Diagnosis Deep Dive and IVIGA human blood donor product made up of immunoglobulins (IgG and IgM antibodies) derived from plasma that can be administered intravenously (IVIG) or subcutaneously (SCIG). For myelin oligodendrocyte glycoprotein antibody disease (MOGAD), it is used as an immunomodulator to reduce disease activity. Sometimes used for acute attacks or as an ongoing preventative treatment./SCIG help: https://mogproject.org/resources/fact-and-information-sheets/
- Clinical TrialResearch studies performed using people as subjects that are aimed at evaluating a medical, surgical, or behavioral intervention to determine to what degree a new treatment (e.g., drugs or medical devices) is safe and effective for general populations. Education: https://mogproject.org/clinical-trials/
- MOGlossary of terms for MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease : https://mogproject.org/resources/moglossary/
- Educational videos and Q&A webinars: https://mogproject.org/resources/podcasts/
- MOGmentum infographic learning series: https://mogproject.org/resources/mogmentum/
- Resources for the Blind and Visually Impaired: https://mogproject.org/resources/for-the-blind/
- Rocket Surveys: https://mogproject.org/rocket-surveys
- Support:
- Support Groups: https://mogproject.org/community/support-groups/
- Connections to Facebook Support Groups: https://mogproject.org/community/connect/
- Community: Stories and Fun Events
- Community Page: https://mogproject.org/community/
- MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. Blog: https://mogproject.org/mog-blog-2/
- Collaborative Partner Resources:
- Siegel Rare NeuroimmuneA term that refers to the components of the immune system that acts in and affects the central nervous system. Association: https://wearesrna.org/
- Guthy Jackson Charitable Foundation: https://guthyjacksonfoundation.org/
- NMO France Association: https://www.nmo-france.org/
- Child Neurology Foundation: https://www.childneurologyfoundation.org/disorder/myelin-oligodendrocyte-glycoprotein-antibody-disease-mogad/
- National MS Society: https://www.nationalmssociety.org/
- MyMyelitis: https://mymyelitis.com/
- International Autoimmune EncephalitisEncephalitis caused by an immune attack on the brain (as opposed to viral encephalitis). Refer to encephalitis. Society: https://autoimmune-encephalitis.org/
Our YouTube Channel: https://www.youtube.com/@themogproject
Rehabilitative & Long-Term Care
Rehabilitation therapy can assist in restoring function, improving QoL, and promoting independence for those living with MOGAD. Starting rehabilitation early following an attack can prevent the complications associated with disuse and addresses functional impairments resulting from neurological damage. Rehabilitation strategies are individualized to the specific symptoms and challenges an individual living with MOGAD is experiencing after an acuteThe severe and sudden onset of a disease process. attack. These specialists make up the multidisciplinary team focused onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. ensuring holistic health for individuals living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease 61.
Physical Therapists
Physical therapists play a vital role in addressing mobility issues such as spasticity, muscle weakness, and pain that result from damage to the central nervous system (CNS)Nerve tissue that resides in and composes the brain, spinal cord, and optic nerve62. This damage can lead to muscle tightness, involuntary contractions, and limited movement63. To help manage these challenges, physical therapists develop personalized exercise programs that focus on stretching and strengthening muscles to improve range of motion and restore functional mobility64,65. They may also recommend assistive devices, like splints, to support weakened muscles and joints65. Pain in MOGAD can stem from neuropathic causes, such as nerve damage that results in burning, stabbing, or shooting pain, or from musculoskeletal issues like spasticity and joint pain caused by immobility63. Physical therapists help manage pain by improving muscle strength and flexibility through targeted exercises64,65. They also use techniques such as massage, stretching, and TENS therapy (Transcutaneous Electrical Nerve StimulationA device that delivers low electrical impulses through a person’s skin. Used to treat some symptoms (such as neuropathy pain or bladder retention) of myelin oligodendrocyte glycoproten antibody disease (MOGAD).) to alleviate discomfort and improve overall function64.Speech and Language Pathologists
Speech and language pathologists are integral in addressing swallowing difficulties and speech impairments that arise when muscles involved in speech and swallowing are weakened or damaged by MOGAD67. Swallowing therapy is provided to help individuals maintain safe swallowing and reduce the risk of choking, often through techniques like thickened liquids or swallowing exercises69. For individuals experiencing speech impairments, speech pathologists offer exercises aimed at improving articulation, breathing, and language skills to enhance clarity and communication69,70.Urologists
Urologists are directly involved in managing bladder dysfunction, bowel dysfunction, and sexual dysfunction, which are common challenges for individuals living with MOGAD78,79. Bladder dysfunction can occur when nerve pathways that control the bladder are impaired, resulting in incontinenceA condition where the muscles or nerves of the bladder (urinary incontinence) or bowel (fecal incontinence) are unable to control or hold its contents. or urinary retention78,79. Urologists help by recommending bladder training, medications such as anticholinergics, and in some cases, catheterization to improve bladder control80. Similarly, bowel dysfunction caused by neurological impairment can lead to constipation or fecal incontinenceA condition where the muscles or nerves of the bladder (urinary incontinence) or bowel (fecal incontinence) are unable to control or hold its contents.79. Urologists recommend dietary modifications, stool softeners, and regular bowel training to manage these symptoms effectively79. Sexual dysfunction, often resulting from nerve damage, can affect sexual arousal and function79,80. Urologists work with individuals to address this through sexual health counseling, medications, and adaptive devices to improve sexual function and quality of life79,80.Occupational Therapists
Occupational therapy helps individuals with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease regain independence in daily activities while addressing specific symptoms such as pain, balance issues, and fatigue65,66. For individuals experiencing musculoskeletal pain or joint stiffness, occupational therapists recommend adaptive tools like reachers or button hooks to reduce strain during tasks such as dressing and eating65,67. They also provide ergonomic strategies to improve comfort and joint mobility67. To address balance problems and mobility challenges, occupational therapists evaluate posture and recommend assistive devices like canes or walkers to improve stability65. They teach safe mobility techniques to reduce the risk of falls and enhance independence68. For those affected by fatigue, occupational therapists guide individuals in energy conservation techniques, helping them prioritize tasks and manage their stamina throughout the day67,68.Neuropsychologists
Neuropsychologists provide valuable support in managing depression, anxiety, and behavioral issues that can result from neurological changes or the emotional burden of living with MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease 32,65. These professionals may help patients cope with mood swings, anxiety, and other emotional challenges, promoting better emotional well-being32. Cognitive impairments, such as memory loss and difficulty concentrating, often occur as a result of brain lesions caused by MOGAD71,72. Neuropsychologists assess these cognitive challenges and develop personalized rehabilitationThe effort of restoring a person back to normal function through targeted treatment such as physical therapy. programs, incorporating techniques to improve attention, memory, and problem-solving skills32. Additionally, behavioral issues such as impulsivity, irritability, or mood swings occur due to damage in the frontal lobes of the brain73. Neuropsychologists use behavioral therapy to address emotional regulation, helping individuals manage and cope with behavioral changes74,75.Neuro-Ophthalmologists and low vision rehabilitationThe effort of restoring a person back to normal function through targeted treatment such as physical therapy. specialists
Neuro-ophthalmologists and low vision rehabilitation specialists are vital members of the healthcare team when it comes to addressing low vision caused by optic nerveThe cranial nerves that relay messages from your eyes to your brain to create visual images. These nerves extend from the retina in the back of the eyes to the part of the brain that processes what we see. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), they may be the target of inflammation or lesions, sometimes causing visual disruption or blindness. damage76,77. These specialists assess the degree of visual impairment using tools like Optical Coherence Tomography (OCT)A noninvasive imaging technology used to obtain high resolution cross-sectional images of the retina. The layers within the retina can be differentiated and retinal thickness can be measured to aid in the early detection and diagnosis of retinal diseases and conditions such as damage causd by optic neuritis in MOGAD. scans and visual field tests to monitor recovery and detect early signs of relapse77. In addition to medical treatment, they recommend assistive devices such as magnifiers, screen readers, and modified lighting to assist with daily tasks like reading and using a computer76. Low vision rehabilitationThe effort of restoring a person back to normal function through targeted treatment such as physical therapy. also involves training individuals in adaptive techniques for safe navigation and performing daily activities despite visual impairments76.Chronic Fatigue Specialists
Chronic fatigue specialists are crucial in managing chronic fatigue, a pervasive issue caused by neurological stress and the burden of living with a chronic illness. These specialists teach individuals how to manage their energy effectively through pacing techniques, improving sleep hygiene, and incorporating stress management strategies to help individuals optimize their daily functioning without overexerting themselves81,82,83. In some cases, medication may also be used to support individuals in managing symptoms and improving their quality of life84.CONCLUSION
While MOGAD is a serious and complex medical condition, ongoing research and clinical trials are making excellent progress toward improved treatment outcomes. With appropriate support, individuals living with MOGAD can maintain or even improve their quality of life (QoL), maximize functional independence, and manage the condition’s complexities. By prioritizing early intervention, personalized treatment plans, and continuous care, individuals with MOGAD can lead fulfilling lives despite the challenges posed by the disease.
References
- cosMOG – About MOGAD. Available from: https://www.cosmogstudy.com/about-mog-ad/. Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. September 30, 2024.
- Elkon and Casali. Nat Clin Pract Rheumtol. 2009; 4: 491-498. Nature and functions of autoantibodies – PMC
- Jeyakumar et al. Eye. 2024;38:2289-2301. springernature_eye_3108 2289..2301
- Harry and Toews. Handbook of Developmental Neurotoxicity. 2007; 87-115. Myelination, Dysmyelination, and DemyelinationThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. – PMC
- Hegen and Reindl. Ther Adv Neurol Disord. 2020;13:1-20. Recent developments in MOG-IgG associated neurological disorders – PubMed
- Gastaldi et al. J Neurol. 2020;267(23):3555-3564. Cell-based assaysA laboratory test used to: • Measure the presence or amount of a specific substance: in a sample, such as blood, urine, or tissue.
• Determine the potency or activity: of a drug or other substance.
• Analyze the purity: of a chemical compound.
• Identify and quantify: biomarkers related to a disease or condition.
for the detection of MOG antibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system.: a comparative study – PubMed - Hor and Fujihara. Front Neurol. 2023;14:1260358. Epidemiology of myelin oligodendrocyte glycoprotein antibody-associated diseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease : a review of prevalence and incidence worldwide – PubMed
- Trewin et al. Autoimmun Rev. 2025: 24: 103693 MOGAD: A comprehensive review of clinicoradiological features, therapy and outcomes in 4699 patients globally – PubMed
- Grant-Peters et.al Ann Clin Transl Neurol. 2021: 8: 1502-1507 No strong HLA association with MOG antibody diseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease in the UK population – PMC
- Ambrosius et al. Int J Mol Sci. 2020;22:100. Myelin Oligodendrocyte Glycoprotein Antibody-Associated DiseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease : Current Insights into the Disease Pathophysiology, Diagnosis and Management – PMC
- Li et al. Front Aging Neurosci. 2022;14:850743. Clinical Features and Imaging Findings of MyelinAn insulating layer, or sheath that forms around nerves, including those in the brain and spinal cord. It is made up of protein and fatty substances. This myelin sheath allows electrical impulses to transmit quickly and efficiently along the nerve cells. If myelin is damaged, these impulses slow down. Oligodendrocyte Glycoprotein-IgG-Associated Disorder (MOGAD) – PubMed
- Jurynczyk et al. Brain. 2017;140:3128-138. Clinical presentation and prognosis in MOG-antibody disease: a UK study – PubMed
- Santoro et al., Ann Clin Transl Neurol. 2023: 10: 672-685. Attack phenotypes and disease course in pediatric MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease – PMC
- Satukijchai et al. JAMA Netw Open. 2022; 5: e2142780 Factors Associated With RelapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). and Treatment of Myelin Oligodendrocyte Glycoprotein Antibody-Associated DiseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease in the United Kingdom – PubMed
- Lopez-Chiriboga et al. JAMA neurol. 2018;75:1355-1363. Association of MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system Serostatus With RelapseWhen you present to your doctor or hospital with new or worsening central nervous system symptoms. Generally, if your symptoms gradually worsen over 24-48 hours, there is heightened concern of a relapse. (Also referred to as a flare by the myelin oligodendrocyte glycoproten antibody disease (MOGAD) community). After Acute Disseminated EncephalomyelitisAn initial and brief autoimmune attack that causes widespread inflammation and damage to the brain, spinal cord, and optic nerve, typically in children. This initial attack establishes the basis for diagnosis. The MOG antibody is detectable in a percentage of Acute Disseminated Encephalomyelitis (ADEM) patients. and Proposed Diagnostic Criteria for MOG-IgG-Associated Disorders – PubMed
- Wendel et al. Neurol Neuroimmunol Neuroinflamm. 2022: 9: e200035 Temporal Dynamics of MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. AntibodiesA protective protein produced by your immune system that attaches to antigens (foreign substances), such as bacteria and toxins, and removes them from your body. In myelin oligodendrocyte glycoproten antibody disease (MOGAD), the body incorrectly produces an antibody that targets myelin oligodendrocyte glycoprotein, a component of the myelin sheath in the central nervous system. in Children With Acquired DemyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. Syndrome – PubMed
- Waters et al. Jama Neurol. 2020;77:82-93.dendrocyte Glycoprotein Antibody Analyses and Outcomes in Children With DemyelinSerial Anti-Myelin Oligoating Syndromes – PubMed
- Asseyer et al. Mult Scler Relat Disord. 2020; 40: 101965. Prodromal headache in MOG-antibody positive optic neuritisInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. – ScienceDirect
- Rempe et al. Mult Scler Relat Disord. 2021; 48:102718. Anti-MOG associated disorder-Clinical and radiological characteristics compared to AQP4-IgG+ NMOSD-A single-center experience – PubMed
- Transverse MyelitisA disorder caused by inflammation of the spinal cord. It is characterized by symptoms and signs of neurologic dysfunction in motor and sensory tracts on both sides of the spinal cord. The involvement of motor and sensory control pathways frequently produce altered sensation, weakness and sometimes urinary or bowel dysfunction. In relation to MOGAD, the inflammation is caused by the MOG Antibody.. Available from: https://www.ninds.nih.gov/health-information/disorders/transverse-myelitis Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. February 2, 2025.
- Filippi and Rocca. White Matter Diseases. 2020: 12: 109-125. Acute Disseminated Encephalomyelitis – PMC
- Shilo et al. Eur J Paediatr Neurol. 2016: 20: 361-367. Long-term motor, cognitive and behavioral outcome of acute disseminated encephalomyelitisAn initial and brief autoimmune attack that causes widespread inflammation and damage to the brain, spinal cord, and optic nerve, typically in children. This initial attack establishes the basis for diagnosis. The MOG antibody is detectable in a percentage of Acute Disseminated Encephalomyelitis (ADEM) patients. – ScienceDirect
- Valencia-Sanchez et al. Ann Neurol. 2022;92:297-302. Cerebral Cortical Encephalitis in Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease – PubMed
- Pace et al. Eur J Neurol. 2024: 32: e16550.Cerebral cortical encephalitis in adults with myelin oligodendrocyte glycoprotein antibody‐associated disease: A national case series – PMC
- Jain et al. Mult Scler Relat Disord. 2021: 49: 102759. “FLAMES: A novel burning entity in MOG IgG associated disease” – PubMed
- Ogawa et al., Neurol Neruoimmunol Neuroinflamm. 2017: 4: e322 MOG antibody-positive, benign, unilateral, cerebral cortical encephalitis with epilepsy – PubMed
- Maturu et al., 2023. Cureus. 2023;15(2): e34994. Unilateral Autoimmune Encephalitis: A Case Report on a Rare Manifestation of Myelin Oligodendrocyte Glycoprotein Antibody Disease – PMC
- Banwell et al. Lancet Neurol. 2023: 22:268-282. Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria – PubMed
- DemyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. Disease. Available from: DemyelinatingThe process in which the protective coating of nerve tissue (i.e. myelin) becomes damaged or breaks down, causing nerve impulses to slow or halt that results in neurological problems. Disease: What It Is, Symptoms & Treatment Accessed February 2, 2025.
- Banks et al. J Neurol Neurosurg Psychiatry. 2022: 92: 384-390. Brainstem and Cerebellar Involvement in MOG-IgG Associated Disorder versus Aquaporin-4-IgG and MS – PMC
- Ladakis et al. Mult Scler J Exp Transl Clin. 2022; 8: 10.1177/20552173221131235. Fatigue is a common symptom in myelin oligodendrocyte glycoprotein antibody diseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease – Dimitrios C Ladakis, Jennifer Gould, Jenny M Khazen, Julia M Lefelar, Scott Tarpey, Charles J Bies, Rebecca Salky, Kathryn C Fitzgerald, Pavan Bhargava, Bardia Nourbakhsh, Elias S Sotirchos, 2022
- Passoke et al. J Neurol Neurosurg Psychiatry. 2024; 333994. Cognition in patients with myelin oligodendrocyte glycoprotein antibody-associated diseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease : a prospective, longitudinal, multicentre study of 113 patients (CogniMOG-Study) – PubMed
- Panginikkod et al., Uhthoff Phenomenon. 2022 OctA noninvasive imaging technology used to obtain high resolution cross-sectional images of the retina. The layers within the retina can be differentiated and retinal thickness can be measured to aid in the early detection and diagnosis of retinal diseases and conditions such as damage causd by optic neuritis in MOGAD. 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing Uhthoff Phenomenon – PubMed
- Forcadela et al. Neurol Neuroimmunol Neuroinflamm. 2023: 11: e200183. Timing of MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system Testing Is Key to 2023 MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease Diagnostic Criteria – PubMed
- Nguyen et al. Mult Scler J Exp Transl Clin. 2024; 10: 2055217241274610. The positive predictive value of MOG-IgG testing based on the 2023 diagnostic criteria for MOGAD – PubMed
- Carta et al. Neurology. 2023: 100: e1095-e1108. Significance of Myelin Oligodendrocyte Glycoprotein Antibodies in CSF: A Retrospective Multicenter Study – PMC
- Redenbaugh et al. Ann. Neurol. 2024: 96: 34-45. Diagnostic Utility of MOG Antibody Testing in Cerebrospinal Fluid – Redenbaugh – 2024 – Annals of Neurology – Wiley Online Library
- Greco et al. J Neurol Neurosurg Psychiatry. 2024: 333554. Clinical, prognostic and pathophysiological implications of MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system detection in the CSFA clear, colorless liquid found throughout the cavities of the central nervous system that helps protect the brain and spinal cord by acting like a cushion against sudden impact or injury, and provides a medium for the transport of nutrients and the removal of waste products for proper functioning.: the importance of intrathecal MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system synthesis | Journal of Neurology, Neurosurgery & Psychiatry
- Sechi et al. Mult Scler. 2021; 27: 303-308. Frequency and characteristics of MRI-negative myelitis associated with MOGA type of protein involved in cell adhesion. Present throughout myelin sheaths. autoantibodies – PubMed
- Jarius et al. J Neuroinflammation. 2016;13:230. MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system in NMO and related disorders: a multicenter study of 50 patients. Part 2: Epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome – PubMed
- Tonev and Momchilova. Biomedicines. 2023;11:328. Therapeutic Plasma Exchange in Certain Immune-Mediated Neurological Disorders: Focus on a Novel Nanomembrane-Based Technology – PubMed
- American College of Rheumatology – Intravenous Immunoglobulin. Available from: Intravenous Immunoglobulin (IVIG) Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. September 30, 2024.
- Spagni et al. J Neuro Neruosurg Psychiatry. 2023; 94:62-69. Efficacy and safety of rituximab in myelin oligodendrocyte glycoprotein antibody-associated disorders compared with neuromyelitis optica spectrum disorder: a systematic review and meta-analysis – PubMed
- Hacohen et al. Jama Neruol. 2018; 75:478-487. Disease Course and Treatment Responses in Children With Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease – PubMed
- Sotirchos et al. Multi Scler Relat Disord. 2022;57:103462 Treatment of myelin oligodendrocyte glycoprotein antibody associated disease with subcutaneous immune globulin – PubMed
- Bruijsten et al. Eur J Paediatr Neurol. 2020;29:41-53. E.U. paediatric MOG consortium consensus: Part 5 – Treatment of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders – PubMed
- Chen et al. Mult Scler Relat Disord. 2022;68:104237. Details and outcomes of a large cohort of MOG-IgG associated optic neuritis – ScienceDirect
- Kiessling. Sci Transl Med. 2017;9: 1208. The FcRn inhibitor rozanolixizumab reduces human serum IgG concentration: A randomized phase 1 study – PubMed
- Sechi et al. Front Neurol. 2022;13:885218. Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease (MOGAD): A Review of Clinical and MRI Features, Diagnosis, and Management – PubMed
- Yamamura et al. N Engl J Med. 2019;22:2114-22124. Trial of Satralizumab in Neuromyelitis Optica Spectrum Disorder | New England Journal of Medicine
- Sheppard et al. Hum Vaccin Immunother. 2017;13:1972-1988. Tocilizumab (Actemra) – PubMed
- METEOROID-A clinical trial to compare satralizumab with placebo, with or without background therapy, in people with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease ). Available from: https://forpatients.roche.com/en/trials/autoimmune-disorder/mog-antibody-disease/a-study-to-evaluate-the-efficacy–safety–pharmacokinet-94806.html Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. September 30, 2024.
- TOMATO- Safety and Efficacy of Tocilizumab in Patients With Myelin Oligodendrocyte Glycoprotein Antibody-associated Disease.Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. September 30, 2024.
- Virupakshaiah et al. J Neurol Neurosurg Psychiatry. 2024;333464. Predictors of a relapsing course in myelin oligodendrocyte glycoprotein antibody-associated disease – PubMed
- Liyanage et al. J Neurol Neurosurg Psychiatry. 2024 95: 544-553. The MOG antibody non-P42 epitope is predictive of a relapsing course in MOG antibody-associated disease – PubMed
- Hyun et al. J Neurol Neurosurg Psychiatry. 2017: 88: 811-817 Longitudinal analysis of myelin oligodendrocyte glycoprotein antibodies in CNS inflammatory diseases | Journal of Neurology, Neurosurgery & Psychiatry
- Whittam et al. J Neurol. 2020;267:3565-577. Treatment of MOG antibody associated disorders: results of an international survey – PubMed
- Kwon et al. JAMA Neurol. 2024; 2811. Time to Treat First Acute Attack of Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease – PubMed
- Levy et al. Mult Scler Relat Disord. 2023;72: 104613 Multiple types of relapses in MOG antibody disease – PubMed
- Said et al. Mult Scler J Exp Transl Clin. 2024;10: 20552173241274605. Quality of life is impaired in myelin oligodendrocyte glycoprotein antibody associated disease – PubMed
- MOGAD Clinic – Overview – Mayo Clinic Accessed onInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement. February 2 2025.
- Rosenthal et al. JIM 2020:68: 321-330. CNS Inflammatory Demyelinating Disorders: MS, NMOSD and MOG Antibody Associated Disease – Jacqueline F Rosenthal, Benjamin M Hoffman, William R Tyor, 2020
- Asseyer et al. Front Neurol. 2020: 11: 778. Pain in NMOSD and MOGAD: A Systematic Literature Review of Pathophysiology, Symptoms, and Current Treatment Strategies – PubMed
- Kubsik-Gidlewska et al. Adv Clin Exp med. 2017: 26: 709-715. Rehabilitation in multiple sclerosis – PubMed
- MOG Antibody DiseaseOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease Information. Available from: MOG Antibody Disease Information – MyMyelitis Accessed on February 2 2025.
- Park et al. Brain Neurorehabil. 2021: 15:e9. Multidisciplinary Rehabilitation for Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-associated Disease: A Case Report – PMC
- Occupational Therapy in Neuro RehabThe effort of restoring a person back to normal function through targeted treatment such as physical therapy.: Restoring Function and Independence. Available from: Occupational Therapy in Neuro Rehab: Restoring Function and Independence. Accessed February 2 2025.
- De-Bernardi-Ojuel et al. Int J Environ Res Public health. 2021: 18:1432. Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review – PMC
- Speech therapy: How it helps in multiple sclerosisAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve.. Available from: Speech therapy for multiple sclerosis (MS): An overview Accessed February 3 2025.
- Tang. J Clin Exp Neuroimmunol. 2024: 9:4. Understanding Aphasia: A Speech Therapist’s Approach to Neurological Disorders
- Risi et al. J. Neurol. Sci. 2025: 470: 123413 Longitudinal assessment of cognitive function in patients with non-relapsing MOG-IgGRefers to the presence of immunoglobulin G (IgG) antibodies in the blood that are specifically targeted against myelin oligodendrocyte glycoprotein (MOG), a protein found in the central nervous system associated disease – Journal of the Neurological Sciences
- Unmet Needs and Challenges Across Pediatric and Adult MOGADOften referred to as MOGAD, Anti-MOG, MOG Ab+, MOG Antibody Disease, MOG Associated Antibody Disease, MOG positive disease Populations. Available from: Unmet Needs and Challenges Across Pediatric and Adult MOGAD Populations. Accessed February 3 2025.
- Understanding and Managing Multiple SclerosisAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve. Mood Swings. Available from: Multiple Sclerosis Mood Swings Explained. Accessed February 5 2025.
- Neurobehavioral Therapy: Transforming Lives Through Brain-Based Interventions. Available from: Neurobehavioral Therapy: Brain-Based Interventions for Mental Health Accessed February 5 2025.
- Turner and Knowles. Fed Pract. 2020: 37:S31-S35. Behavioral Interventions in Multiple Sclerosis – PMC
- Optic NeuritisInflammation of the optic nerve that may be classified as unilateral (affecting one eye) or bilateral (affecting both eyes) that may result in vision changes, vision loss, and/or pain with eye movement.: How Long for recovery? Available from: Optic Neuritis: How Long for Recovery? – Eye Surgery Guide Accessed February 5 2025.
- What is a Neuro-Ophthalmologist? Available from: What Are the Diseases Treated by Neuro-Ophthalmologists? Accessed February 5 2025.
- Li et al. Neurology. 2020: 95: e2924-e2934. A clinico-neurophysiological study of urogenital dysfunction in MOG-antibody transverse myelitis – PubMed
- DasGupta and Fowler. Therapy in Practice. 2003: 63: 153-166. Bladder, Bowel and Sexual Dysfunction in Multiple Sclerosis | Drugs
- Bientinesi et al. Int neuronal J. 2020: 24: 118-126. Managing Urological Disorders in Multiple Sclerosis Patients: A Review of Available and Emerging Therapies – PMC
- Pacing: Mastering your energy to manage chronic illness. Available from: Pacing: Mastering your energy to manage chronic illness better – Carenity Accessed February 5 2025.
- Gupta et al. BMJ Open. 2023: 13:e060401. Sleep hygiene strategies for individuals with chronic pain: a scoping review – PMC
- Fatigue in the Context of MSAn autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve.. Available from: MS and Fatigue Fact Sheet | Cleveland Clinic. Accessed February 6 2025.
- Multiple Sclerosis (MS)An autoimmune disease that attacks healthy cells in the myelin, the protective sheath that surrounds nerves in the central nervous system (CNS) leading to neurological symptoms originating from the brain, spinal cord, and/or optic nerve. and Sleep. Available from: MS and Sleep Disturbances: Insomnia, Nocturia, & Coping | Sleep Foundation. Accessed February 6 2025